Here is the song I hear from medical professionals in every developed country I have visited over the last several years and from delegates of countries who have come to Boston to explore ideas. I hear about the same demographic trends. There are three cohorts: (1) The elderly, who are living longer than ever, whose diseases -- even cancer -- are chronic in nature, requiring supervision, ongoing diagnosis, expensive drugs and often hospital-based treatment; (2) The baby-boomers, the entitled children of the 1940s and 1950s, who are just entering the age of hospitalization for serious diseases and who believe they have the right to elective procedures for aches, pains, and conditions that prior generations would have just lived with; and (3) The next two generations, often sedentary and malnourished, who are obese and developing life-long sequelae from unhealthy lifestyles.
In those countries with long-standing national health systems, which have properly emphasized the importance of primary care, I see a tendency to adopt the "rule of rescue" and otherwise believe that their tertiary treatment needs to be on par with the US. They are prepared to invest millions in facilities and equipment to make this so.
Meanwhile, the US is about to start catching up with the world by providing access to care and especially primary care. For the foreseeable future, as people begin to have the kind of early diagnostic testing they deserve, there will actually be an increase in their health care expenditures. Conditions which would have laid dormant until the patient presented in the Emergency Department will instead be discovered sooner, requiring intervention and treatment.
In all countries, I see the medical-industrial complex at work, inventing new approaches to diagnosis and treatment. These approaches will often meet FDA-like regulatory approval for safety; but they will not be judged for relative efficacy. Doctors, particularly those in academic medical centers and other prestigious or ambitious hospitals, will demand the acquisition of these devices and drugs. They will not be drawn to them by cost-effectiveness. They will acquire them because they are the latest, because they want to keep up with the competition, and because they believe them to be necessary to gain market share. They -- abetted by direct-to-consumer advertising -- will help convince their patients that they need these new devices and drugs. In short, perceived reputation will often outweigh efficacy in the value equation.
These factors are compounding each other's impact to lead every developing country to an unsustainable increase in health care costs.
All of this is not going on without notice to the people who pay the bills -- the government, the insurance companies, and/or the employers. They are putting pressure back on the system, but they use methods that are crude and unproven. Medicare, for example, will focus on "never events," penalizing institutions as though those institutions want never events to occur. Others repeat the religious dogma of capitation, while providing no evidence that capitated systems have produced the desired result. Accreditation agencies focus on minutia, checking off their own checklist with no cognizance of the cost impact brought about by nitpicking that distracts from real process improvement. In national health systems -- and incipient in the US, too -- parallel systems of high-end insurance products are offered to those who can afford them. These products reduce equity in countries for whom equity and solidarity has always been important, but give the government an "out" in the provision of premium service.
Meanwhile, I hear of insufficient attention to things that can be designed and driven by the medical profession to make a difference in the cost trend while supporting the needed dimensions of care -- those items I put up at the upper right corner of this blog: Patient-centered care, eliminating preventable harm, transparency of clinical outcomes, and front-line driven process improvement. I summarized this approach several weeks ago. I'm not go to play that old song again here, but you can check back and read it if you like. I will repeat the conclusion:
To the extent the medical profession continues to abdicate responsibility, the more will step in politicians, regulators, and payers to do it for them. If you are a doctor and already feeling a lack of control over your professional life and your relationship with your patients, just wait.
But I was reminded of another point last week in Denmark. Part of taking control is to ask for help, and you folks need help from other industries and fields that have learned to deal with structural change and process improvement. You can't keep saying, "But we are different." Everyone is different. Teach them what they need to know so they can teach you want you need to know. It was great to see that the folks at the Copenhagen conference have accepted that. Here is the result to the question of whether they thought they ought to bring in people from other industries to help achieve their goals.
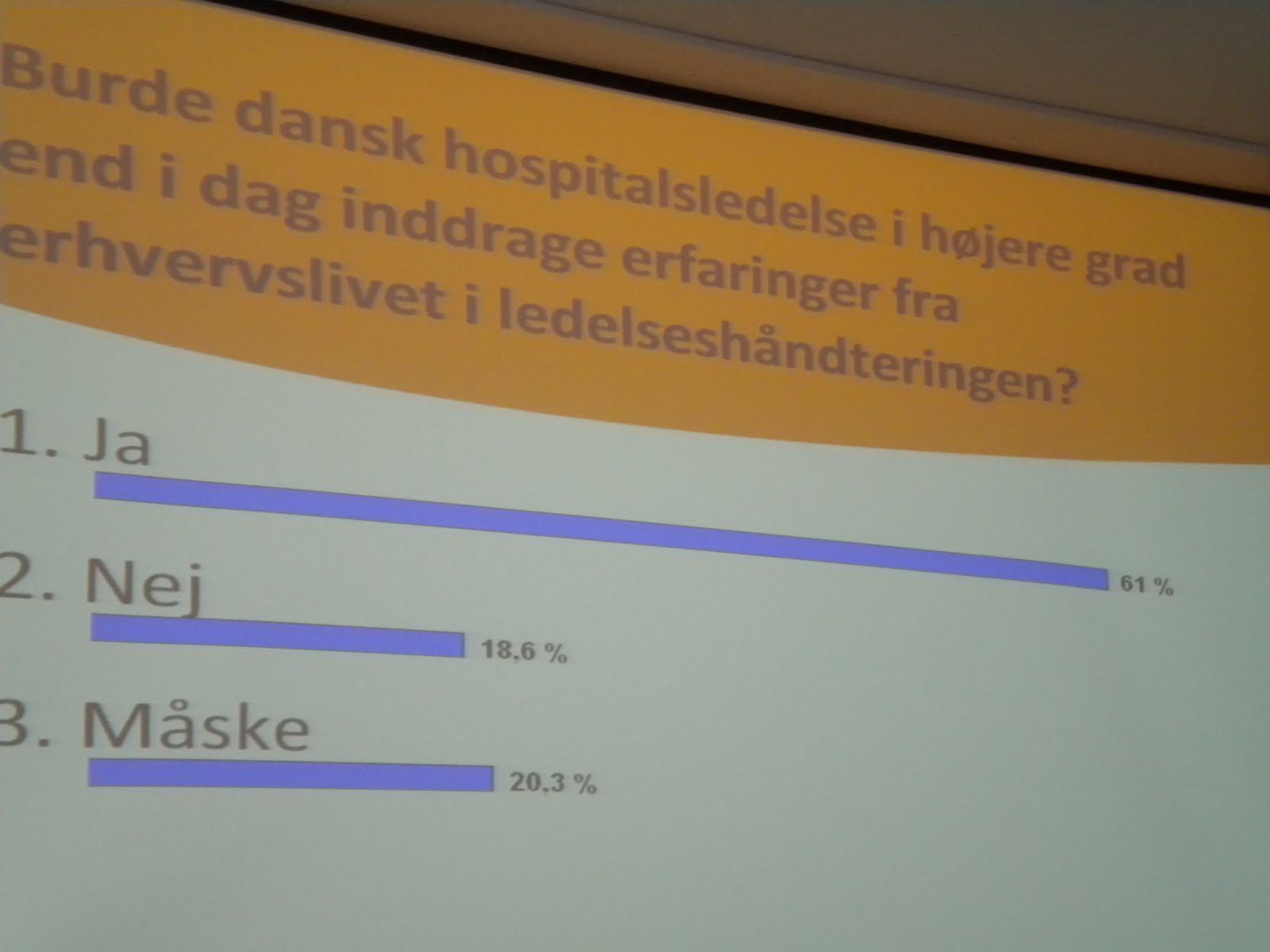
"Ja" is definitely the right answer. It is a demonstration of the intellectual modesty needed to make progress.
If you have made it this far, you have probably heard enough from me today. Just for entertainment, here's the actual song.
Click here if you can't see the video.
No comments:
Post a Comment